
Newsletter May 2026
Abortion pills in the crosshairs… again
Abortion pills were back at the Supreme Court of the United States this month. That’s never a good thing with the majority on this Supreme Court! but we are fine−for the moment at least.

Credit: Hey Jane
Did you know abortion pills are now the main method of abortion in the U.S.?
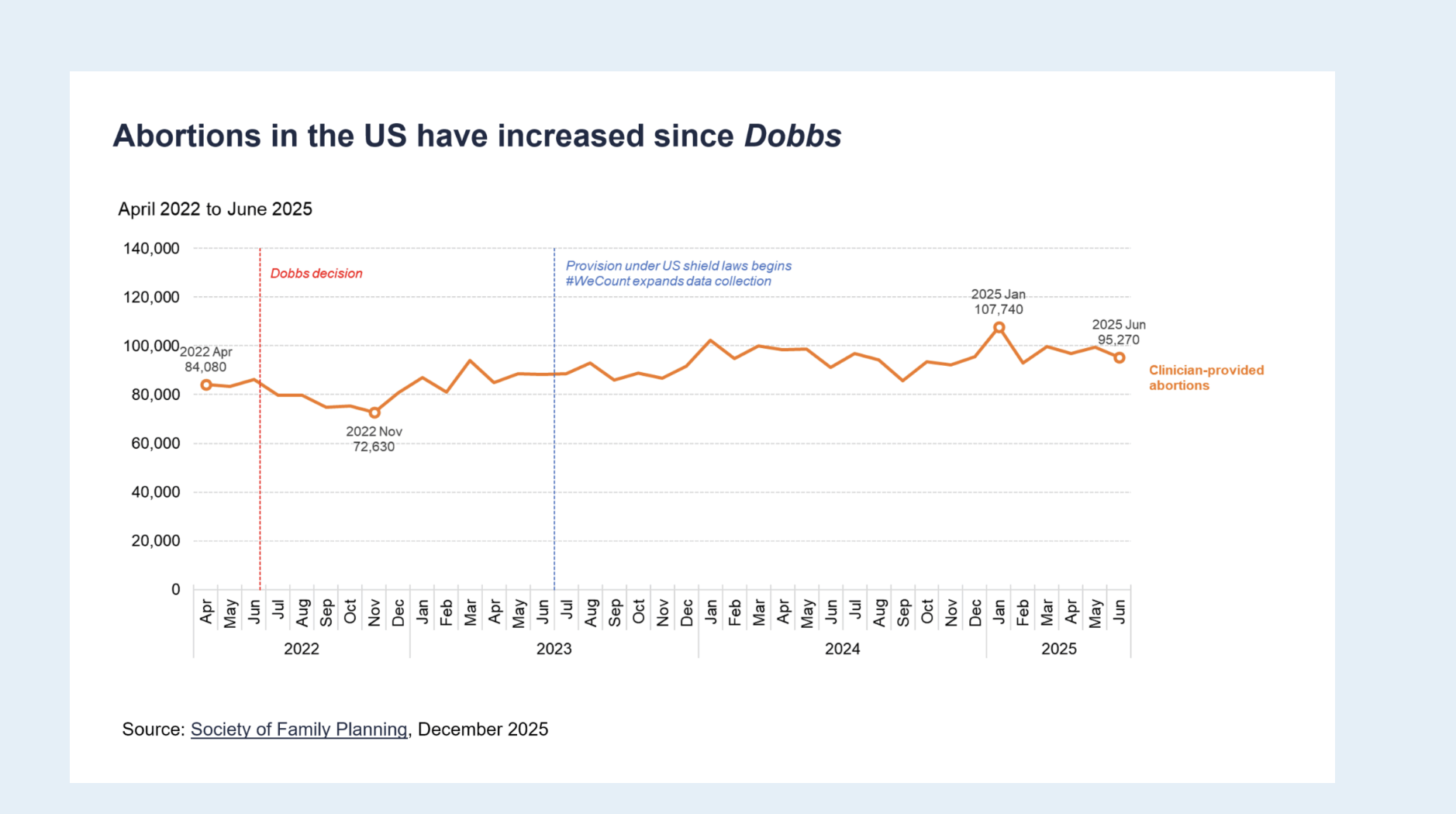
According to the Guttmacher Institute, there were an estimated 1,126,000 abortions provided by clinicians in the U.S. in 2025. Of these, at least 63% were carried out with pills. And, by the end of 2024, 25% of all abortions were done via telehealth/pills mailed to the patient. That figure was only 5% in June 2022, when the Supreme Court overturned the constitutional right to abortion in Dobbs v. Jackson Women’s Health Organization.In fact,
In fact, Dobbs arguably caused the rise of abortion pills in the U.S. True, Dobbs allowed conservative U.S. states to enact restrictive laws to shut down abortion clinics. But this wasn’t 1973 anymore, when Roe v Wade was decided. We now have abortion pills, telehealth and the Internet.
In the U.S., a two-drug combo (mifepristone followed by misoprostol) is commonly used to induce abortion. Telehealth prescribing and mailing of abortion pills was first allowed by the Food and Drug Administration (FDA) in 2021 during COVID and subsequently formally authorized by the agency in 2023.
When Dobbs came down, abortion providers, activists and advocates ramped their plans to provide abortion pills to patients through the mail. Pregnant persons turned to trusted websites like Plan C to obtain information about abortion pills. Concurrently, a number of progressive states (including Massachusetts, Colorado, California and New York) adopted robust “shield laws” that protect health providers who prescribe and ship abortion pills to restrictive states. The laws shield these providers by blocking subpoenas and extradition requests by restrictive states.
This has been a game changer. It has allowed tens of thousands of pregnant persons to self-manage their abortions at home, no matter where they live. The pills are a main reason why, even after Dobbs, the number of abortions in the U.S. went up rather than down.
Now, we can’t downplay the harm caused by Dobbs. Pregnant persons living in the 17 U.S. states with total or quasi-total abortion bans who need or choose in-person care have to travel further than before, often at great expense. And those who need emergency care during pregnancy because they’re experiencing a miscarriage or pregnancy complication are suffering injuries or actually dying because doctors are afraid or unable to intervene to save them. It’s absolutely terrifying.
At the same time, by June 2025, under shield laws, 14,770 packs of pills/month (i.e. approximately 55% of all telehealth abortions) were provided to people living in states with abortion bans, with that share growing, according to the #WeCount project of the Society of Family Planning. Abortion pills by mail have, paradoxically, made access to abortion easier and more affordable in many more settings than before Dobbs.
Anti-abortion actors have been very unhappy with this state of affairs. This wasn’t the plan! So they have turned to lawsuits. Their courtroom tactics are two-fold: 1) attacking the FDA review and approval of mifepristone, and 2) suing the brave abortion providers who are prescribing and mailing mifepristone out-of-state.
We shouldn’t be surprised. Mifepristone has been in the crosshairs of anti-abortion activists for decades. This current assault is led by Alliance Defending Freedom (ADF), an evangelical Christian legal group well known for its virulent anti-gender and anti-reproductive rights litigation. Erin Hawley, ADF’s general counsel, is married to U.S. Senator Josh Hawley (Republican of Missouri). In March 2026, Senator Hawley proposed legislation (the Safeguarding Women from Chemical Abortion Act) to ban mifepristone on the grounds that it is dangerous to women and likely to be abused. Hawley’s bill would allow women to sue mifepristone’s manufacturers for the “harms” the drug has caused them. It’s a Hawley family affair…


Suing the FDA
All medication sold in the U.S. requires approval by the FDA, which is granted after detailed review by experts. The FDA process has long been considered a gold standard for drug approval worldwide, and it has been predictable and scientifically driven.
Mifepristone was approved for abortion by the FDA in 2000, after an extensive review. It’s important to note that, in 2000, even though mifepristone already had an excellent safety record, the FDA attached REMS (Risk Evaluation and Mitigation Strategies), i.e. restrictions to its prescription and distribution. REMS are measures usually imposed on drugs with serious safety concerns, such as thalidomide or fentanyl, and they mandate steps such as physician or pharmacy certification, patient monitoring, or restricted distribution. Out of over 20,000 drugs approved for sale the U.S., only 74 are subject to REMS. Mifepristone didn’t belong in that group, but extreme caution (and fear of anti-abortion actors?) apparently guided the FDA at the time.
The evidence on mifepristone called for a change. In 2016, the FDA allowed nurses (and not only doctors) to prescribe mifepristone, and the drug was authorized for use through the 10th week of pregnancy. When the FDA formally allowed remote prescription and dispensing of mifepristone in 2023 (it had informally allowed it since 2021 during COVID) , it relied on 23 years of safety data from over seven million uses in the U.S., as well as many million more in Europe and beyond since the 1980s. In fact, mifepristone’s outstanding safety record—it is associated with fewer deaths and injuries than Viagra or Tylenol—actually argues for it to be available over the counter. And needless to say, mifepristone is vastly safer than pregnancy itself!
Despite this, the ADF and its acolytes in repressive states are determined to prove that mifepristone is dangerous. To that end, they’ve claimed the FDA was mistaken when it first approved it and subsequently relaxed its controls over it. It’s absolutely contrary to the evidence, but science has never stopped anti-abortion activists. They have launched several such (so far unsuccessful) lawsuits against the FDA and mifepristone since 2023.
The latest legal saga began on May 1, when in State of Louisiana v. Food and Drug Administration (FDA), the ultra-conservative U.S. Court of Appeals for the Fifth Circuit (which decides appeals from Texas, Louisiana and Mississippi) suddenly banned telehealth prescribing and mailing of mifepristone nationwide. The Fifth Circuit ruling would have forced pregnant persons across the U.S. to travel to a certified clinic or certified doctor’s office to be handed mifepristone in-person. This would have affected abortion access even in states where abortion is legally protected and telemedicine access is allowed. It also would have limited mifepristone access for indications other than abortion, such as miscarriage management, uterine fibroids and Cushing syndrome.
Louisiana argued the FDA had used flawed or nonexistent data to allow mifepristone to be prescribed and distributed remotely. Incidentally, Louisiana never filed a citizen petition, the prescribed process for asking the FDA to take certain action such as additional safety testing. It went straight to a lawsuit.
Louisiana also claimed that the prescribing and shipping of mifepristone by out-of-state health providers negated its ban on abortion (more on that below). Additionally, Louisiana claimed it had to pay $92,000 in Medicaid bills for two pregnant women who suffered complications allegedly caused by mifepristone and that, therefore, Louisiana could dispute the FDA rules that allowed mifepristone to be mailed to Louisiana women. (That’s what courts call a “speculative” and “attenuated” chain of causation if I ever saw one). An additional plaintiff, Louisiana resident Rosalie Markezich, claimed she was forced to take mifepristone against her will by her abusive boyfriend (why this should lead to the banning of mifepristone nationwide rather than the boyfriend’s arrest, is an open question!)
In a court acting in good faith, I don’t see how these arguments could ever result in immediate, nationwide action on mifepristone. But the Fifth Circuit enthusiastically went along with it and granted the suspension Louisiana requested.
In a New York Times article published May 7, 2026, entitled Did This Appeals Court Go Rogue on Abortion Pills?, a Trump 1.0 Department of Justice official called this Fifth Circuit’s decision “Bonkers Town-adjacent,” if not “full Bonkers Town.” But then again, the Fifth Circuit is bonkers. It's so extreme that it's regularly overturned by the uber-conservative Supreme Court of the United States: in 2025, 10 of its 13 decisions that reached the Supreme Court were overturned.
(In 2023, the Supreme Court actually tossed out a very similar Fifth Circuit ruling on mifepristone, in Alliance for Hippocratic Medicine v. FDA (discussed in a previous Newsletter), because it found that the plaintiffs, a group of anti-abortion doctors incorporated in Texas just before the case was filed, didn’t have standing, i.e. a valid reason to sue the FDA.)
DANCO and GenBioPro, two U.S. manufacturers of mifepristone, turned to the Supreme Court to overturn the May 1 suspension, while hundreds of experts and “friends of the Court” (including progressive U.S. states, members of Congress, abortion providers, reproductive rights groups, medical organizations, and the pharmaceutical lobby group Pharmaceutical Research and Manufacturers of America (PhRMA)) filed briefs to defend the FDA process.
Was the right-wing majority on the Supreme Court going to overturn the Fifth Circuit and allow remote dispensing of mifepristone to continue, or would it seize this opportunity to deal a major blow to abortion access across the country? It didn’t help that Samuel Alito, the far-right Justice who authored Dobbs, is the Justice assigned to appeals coming from the Fifth Circuit and was therefore the one to receive this case. On May 4, Alito paused the Fifth Circuit order while the parties prepared their arguments. This restored telehealth access to mifepristone for a week. He then extended the pause to May 14. On that day, the Supreme Court finally suspended (‘stayed’) the Fifth Circuit’s order, with Justices Alito and Clarence Thomas dissenting vehemently. Patients across the U.S. could continue to access mifepristone by telehealth and mail for now.
It was a white-knuckle experience. As noted by The Guardian, “On Thursday [May 14], the confusion and chaos around mifepristone access was encapsulated in the roughly 30-minute period when Justice Samuel Alito was late on the deadline he’d given himself to deliver a decision – allowing the stay to expire and temporarily creating a nationwide ban on mail-order mifepristone.”
And this particular battle isn’t over: the case is now back in the Fifth Circuit for a full briefing and argument and will likely return to the Supreme Court after that. It’s far from certain this Supreme Court majority will support ongoing, convenient, evidence-based access to mifepristone.
You’ll agree with me this is no way to handle essential medications!
But one thing the swift reaction to the Fifth Circuit ruling showed, was that abortion providers and advocates were ready. While some providers stopped their telehealth abortion services, others immediately switched to the alternative (also safe and effective) misoprostol-only regimen, which wasn’t affected by the ruling. And the coordinated legal and media response by the broad abortion rights community was something to behold.
What should we expect now? There are reasons to worry.
For starters, the FDA in the second Trump Administration appears to be wavering under political pressure, and not only on abortion. After the FDA received letters from anti-abortion organizations and right-wing state attorneys general, Secretary of Health and Human Services (HHS) Robert F. Kennedy Jr and FDA Commissioner Marty Makary announced in September 2025 that the FDA was conducting a comprehensive review of mifepristone safety and of the 2023 REMS, something completely unnecessary…unless of course the goal is to find fault with mifepristone.

The FDA announcement of the review was itself very damaging. In their letter, Kennedy and Makary wrote: “HHS’s decision to do so is informed by the lack of adequate consideration underlying the prior REMS approvals, and by recent studies raising concerns about the safety of mifepristone as currently administered.” [my emphasis] The FDA letter also pointed to “studies” on the dangers of mifepristone carried out by the Ethics and Public Policy Center, a DC-based far-right “institute working to apply the riches of the Jewish and Christian traditions to contemporary questions of law, culture and politics…"
Unsurprisingly, the Fifth Circuit in Louisiana jumped on that FDA letter in its ruling reinstating the REMS. Also very concerning is the fact that, in the Supreme Court this month, the FDA didn’t bother to submit a brief to defend itself and its own process.
The FDA “review” of mifepristone will presumably materialize at some point, and if carried out under the influence of anti-abortion actors, could be very problematic. Incidentally, Trump-appointed FDA Commissioner Marty Makary ”resigned” three weeks ago, in part because anti-abortion forces were accusing him of slow-walking that mifepristone review.
We can only imagine what mayhem this kind of interference will cause in the drug development and approval process if it becomes the new normal. Would we face state-by-state challenges of drugs and vaccines anytime an ideologically minded governor or legislature decided to launch an attack? What’s next? Hormonal therapy, birth control, mRNA technologies? That is why medical associations and the pharmaceutical industry have raised such concerns about these preposterous lawsuits.
I’m also shaking my head at the fact that a court would impose prescription and dispensing restrictions on a medicine in direct contradiction of an FDA decision. That’s an incredible level of meddling in scientific decision-making. Courts of law are not well suited for reviewing the validity of the detailed scientific evidence used to evaluate the safety and efficacy of drugs. That's why Congress assigned this role to a specialized agency. As DANCO states in its brief to the Supreme Court in Louisiana: “The Fifth Circuit’s decision is unprecedented: Until now, no federal court has ever immediately commanded a drug revert to conditions of use that FDA has found are unwarranted under the REMS statutory framework.”
It’s not the only such medical and scientific outrage the two Trump Administrations have subjected us to, but it should worry us deeply. Banning or severely restricting an effective, safe, essential medicine that over 600,000 persons take every year in the U.S. would cross another frontier.
And Justice Clarence Thomas’ dissent in Louisiana gives us another cause to worry. He called the mailing of mifepristone a “criminal enterprise,” citing the 1873 federal anti-obscenity Comstock Act (regrettably never repealed), which criminalized the mailing of drugs or instruments used for abortion. This could be the ADF’s (and the Supreme Court’s) next avenue against the 2023 REMS and the mailing of abortion pills.
Suing out-of-state abortion providers
The other tack has been to sue the brave health providers who prescribe and mail abortion pills to persons living in restrictive states.
In 2025, Louisiana criminally indicted Dr Margaret Carpenter of New York for providing abortion pills to Louisiana women, and Jeff Landry, the governor of Louisiana, signed a warrant for her extradition. Governor Kathy Hochul of New York said no and reminded him of her state’s shield law. Meanwhile, Texas sued Dr Carpenter in civil court for more than $100,000 and ordered her to stop mailing pills to Texas. Dr Carpenter has not replied to either lawsuit or complied with their requests. In 2026, Louisiana stepped up its efforts, this time criminally indicting Dr Rémy Coeytaux of California. Governor Gavin Newson of California said he would refuse to extradite Dr Coeytaux. Texas also sued Debra Lynch, a Delaware nurse practitioner, so far to no avail. Shield laws are proving effective for the moment, but these laws could also be challenged all the way to the Supreme Court as the battle among states intensifies.
GenBioPro and DANCO noted (with a note of sarcasm) in their Louisiana brief to the Supreme Court that: “the alleged frustration of Louisiana’s laws occurs because other states have enacted ‘shield laws’ to protect medical practitioners in their states from extradition for prescribing mifepristone. This difference in state policies is yet again a natural result of this Court 'return[ing]' abortion policy to the states,” in the Dobbs ruling.” That’s right… We had a uniform abortion policy nationwide with Roe v Wade. We now have different criminal abortion laws in different states, and California doesn’t have to defer to Louisiana’s abortion ban.
As 19 progressive states and the District of Columbia stated in their amicus brief: “the Fifth Circuit improperly elevated the policy preferences of States that have banned or restricted abortion over the preferences of other States that have made the different but equally sovereign determinations to promote access to abortion care.” Or as phRMA argued: “[Louisiana] would have no authority to sue to block individuals and entities outside its territory from engaging in activity that is legal where it occurs.” States’ rights, y’all.
In February 2025, I interviewed the brilliant Dr Angel Foster on the FMUS podcast. Under the Massachusetts shield law, Dr Foster and her colleagues at the Massachusetts Medical Abortion Project (The MAP) provide abortion care via telehealth to about 3,000 pregnant persons a month across the U.S. Dr Foster hasn’t been sued so far, but she is cautious. She told me she never drives a car outside Massachusetts and doesn’t travel to or through states with abortion bans. Those are serious personal inconveniences. Moreover, The MAP’s operations are structured to ensure that no single individual on the team can be associated with the entire act of providing abortion pills: different people take the orders, handle the payment and package and mail the pills.
These courageous providers live with these risks to safeguard women’s health and lives—risks they should never have to take.
The future of abortion pills
When I asked Dr Foster whether abortion pills could ever be suppressed in the U.S., she had these words of hope:
“That ship has sailed! Even if all the shield law practices had to close down, medication abortion access will continue in the U.S. There are international providers that can send pills, there are new innovative strategies like community health networks that distribute pills in the South. It might take a little longer, it might be more expensive, we might have to think of other strategies, but pills are not going away even if the FDA re-regulates mifepristone. And we have misoprostol, which can be used alone and is a wonderful alternative.”
In a recent interview in the New York Review of Books, journalist Amy Littlefield agreed with this, and highlighted the huge change underway: “Renee Bracey Sherman, a reproductive justice activist, has a saying: “Everyone loves someone who’s had an abortion.” Two thirds of abortions in the United States now are happening with medication, and so a lot of us now love someone who has had a medication abortion. That will undermine efforts by the anti-abortion movement to argue that these drugs are ineffective or dangerous. Meanwhile, a website like Plan C Pills, where people can find information about medication abortion, is becoming a kind of household name. One of my favorite stats… is that Plan C Pills has circulated close to five million stickers [about abortion pills]. Someone who uses a restroom at a bar in, you know, Tuscaloosa might look up and see a sticker on the wall. That kind of cultural change and awareness is really hard to reverse no matter what the courts do.”

That is my opportunity to remind you that advance provision of abortion pills is an option many more people should use. You simply order abortion pills to keep in your medicine cabinet in case you, or someone you love, might need them. You know, like other medicines you keep at home in case of need!
Go to Plan C, which will direct you to advance providers, including The MAP, Women on Web and Aid Access. Planned Parenthood also recently announced that they too will, for the first time, offer advance provision via telehealth and in person in Hawai’i and Washington State. That's great news. Planned Parenthood hasn’t been a pioneer on abortion pills, but we welcome them to the revolution.
And if you’d like to make a donation to The MAP (they subsidize the pills for those who can’t afford them), click on https://secure.actblue.com/donate/themap or email admin@chrcmap.org.
A luta continua!
In feminist solidarity for reproductive justice and freedom,
FG